Gumboro Disease: The Variant The Silent Enemy

Vaccination is a veterinary medical procedure with major sanitary, economic, and zootechnical implications. Even when performed by field operators, it remains under the responsibility of the veterinary practitioner, who determines its indication, validates the practical procedures, and monitors the quality of execution.
In laying hens and future laying pullets, the objective of a vaccination audit is to secure the entire operational chain: vaccine storage, organization of the vaccination process, preparation of equipment, reconstitution of solutions, team allocation, technical execution, waste disposal, and documentation traceability.
A rigorous audit helps identify deviations that may compromise flock immunization: wrong vaccine selection, incorrect dilution, temperature failure, poor water quality, inappropriate vaccination technique, poor restraint, missed birds, or incomplete post-vaccination control. Success therefore depends not only on the vaccine itself, but on the overall control of the entire process.
Cross-cutting points to verify during an audit include vaccine stock management, batch compliance, respect of the cold chain, operator competence, cleanliness and maintenance of equipment, diluent quality, recording of timing, allocation of responsibilities, control of vaccine uptake, and archiving of field observations.
A- Vaccination via Drinking Water
This route is mainly used in future laying pullets, particularly for certain live vaccines such as Gumboro and, less commonly, avian encephalomyelitis. Its main advantage lies in the ability to vaccinate a large number of birds rapidly, provided that water effectively serves as a carrier without altering the vaccine virus.
The most common causes of failure are well known: poorly stored or frozen vaccine, wrong dose, expired vaccine, product confusion, failure to neutralize chlorine, excessive or insufficient water volume, residual water remaining in the system, water deprivation that is too short or too long, excessive stocking density, poor team coordination, and poor flock health status.

Priority audit points:
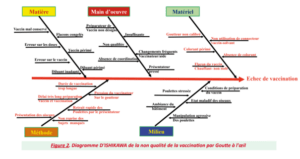
B- Eye-Drop Vaccination
Eye-drop vaccination is a reference technique for several respiratory diseases, particularly infectious laryngotracheitis (ILT). Its strategic value lies in the fact that it best reproduces the natural route of infection through the conjunctiva, thereby promoting targeted and homogeneous vaccine uptake.
In the case of ILT, this technique helps avoid the limitations associated with other routes, especially drinking water or certain spray administrations, whose efficacy on the target mucosal surfaces may be inconsistent. Poor vaccine coverage leaves susceptible birds within the flock and favors circulation of the vaccine virus among insufficiently immunized animals.
The apparent simplicity of eye-drop administration should not obscure its technical demands. The choice of diluent, storage temperature, proper reconstitution, and correct use of the dropper directly determine the success of the operation.
Common deviations include incompatible diluent use, storage errors, irregular drop size, failure to wait for absorption, team fatigue, vaccine warming, and insufficient uptake control.
Priority audit points:
C- Wing-Web Vaccination
Wing-web vaccination is used mainly against fowl pox, often in association with avian encephalomyelitis, and may also be applied in breeders for certain specific indications. This technique requires excellent process organization because the expected success rate must be very high.
Three factors explain this requirement:
The audit must therefore focus as much on the quality of the technique as on the efficiency of the collective organization.
Preparation begins with verifying compatibility between the vaccine and the diluent, followed by careful reconstitution and rational distribution of the vaccine volume among operators. This reduces vaccine warming and limits interruptions. Equipment must be inspected before starting: wing-web needles must be clean, functional, and not deformed, and automatic applicators must be perfectly tight when used.

Priority audit points:
D- Intramuscular Vaccination
The intramuscular route is reserved for inactivated vaccines, most often oil-based. It is of major importance because, unlike live vaccines, these products do not multiply in the body; therefore, any injection failure is equivalent to an absence of effective protection for the bird concerned.
Inactivated vaccines have a complex formulation combining antigen, aqueous phase, and oil adjuvant. Their homogeneity is a critical point. Inadequate storage, especially freezing, may irreversibly alter the structure of the emulsion and reduce immune efficacy.
This technique also involves occupational risks. Accidental self-injection into fingers is a known and sometimes serious incident, justifying specific training, strict safety procedures, and the availability of a clear response protocol. From the animal perspective, a poorly positioned injection may lead to sequestration of the vaccine in the muscle, inadequate diffusion, or local lesions detrimental to both efficacy and welfare.
Frequently encountered errors include improper storage, vaccine freezing, emulsion heterogeneity, incorrect volume adjustment, inappropriate needle selection, inadequate restraint, and failure to respect the correct anatomical injection site. Detailed audit sheets are particularly useful to break down each step and objectively identify non-conformities.

Priority audit points:
E- Subcutaneous Vaccination
Subcutaneous injection is an alternative to the intramuscular route, particularly in young birds with insufficient muscle mass, but also in certain situations involving older birds. It allows administration of various injectable vaccines while limiting some of the constraints associated with the muscular site.
The injection site must be strictly respected: the posterior part of the neck, at the middle third, by lifting the skin between the thumb and index finger. This maneuver creates a suitable subcutaneous space and allows proper perception of product delivery. Poor localization may result in intradermal injection, accidental intramuscular delivery, or product reflux.
Final quality depends less on the route chosen than on the discipline applied at each

Priority audit points:
Conclusion
A vaccination audit in laying-hen production should not be regarded as a mere control formality, but as a tool for sanitary management and performance improvement. It transforms a set of sometimes empirical practices into a standardized, measurable, and improvable procedure.
Whatever the administration route, the same principles apply: product quality, proper storage conditions, rigorous preparation, clear organization of the process, operator competence, veterinary supervision, real-time quality control, and complete traceability. Prevention of vaccination failure therefore depends first and foremost on the quality of execution.